Emmetropic Eye
Emmetropic Eye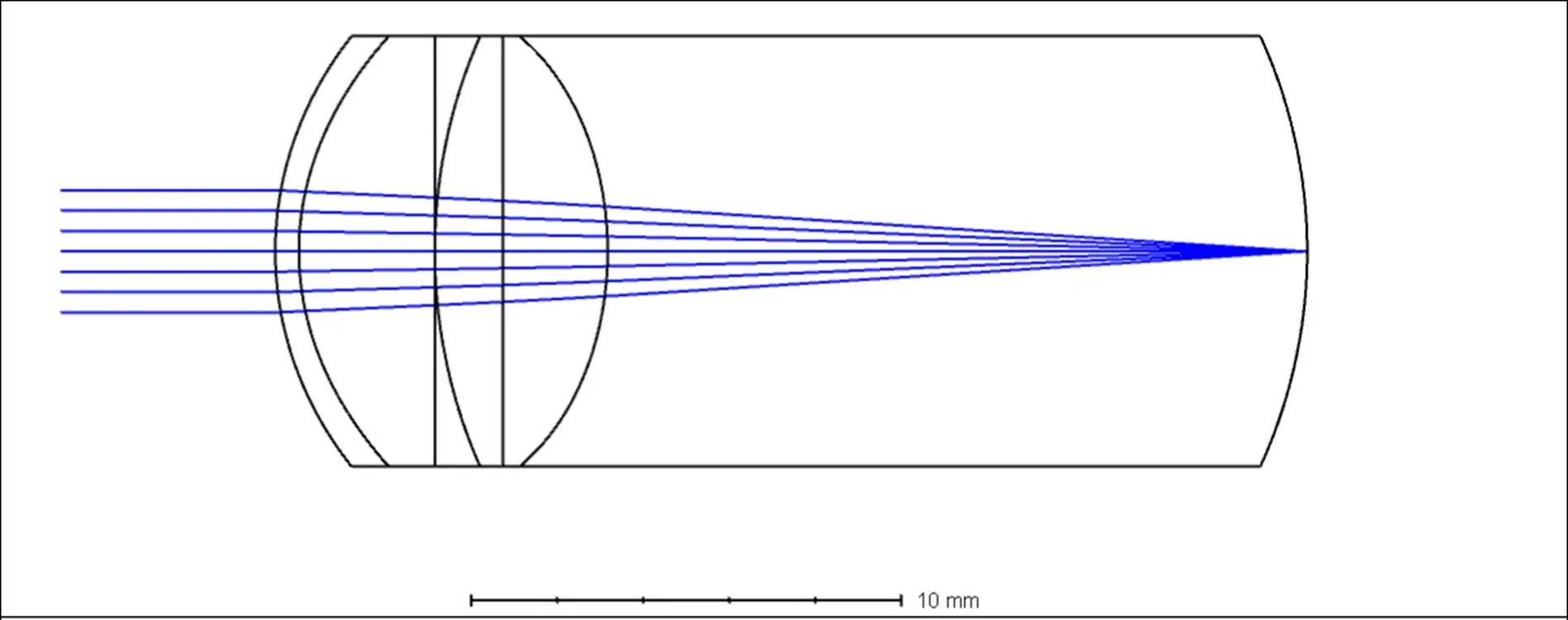
In a "normal" eye, parallel light rays coming from far away objects are refracted by the cornea and lens and then focused precisely onto the retina. This allows clear vision for distant objects.
Myopic Eye
Myopic Eye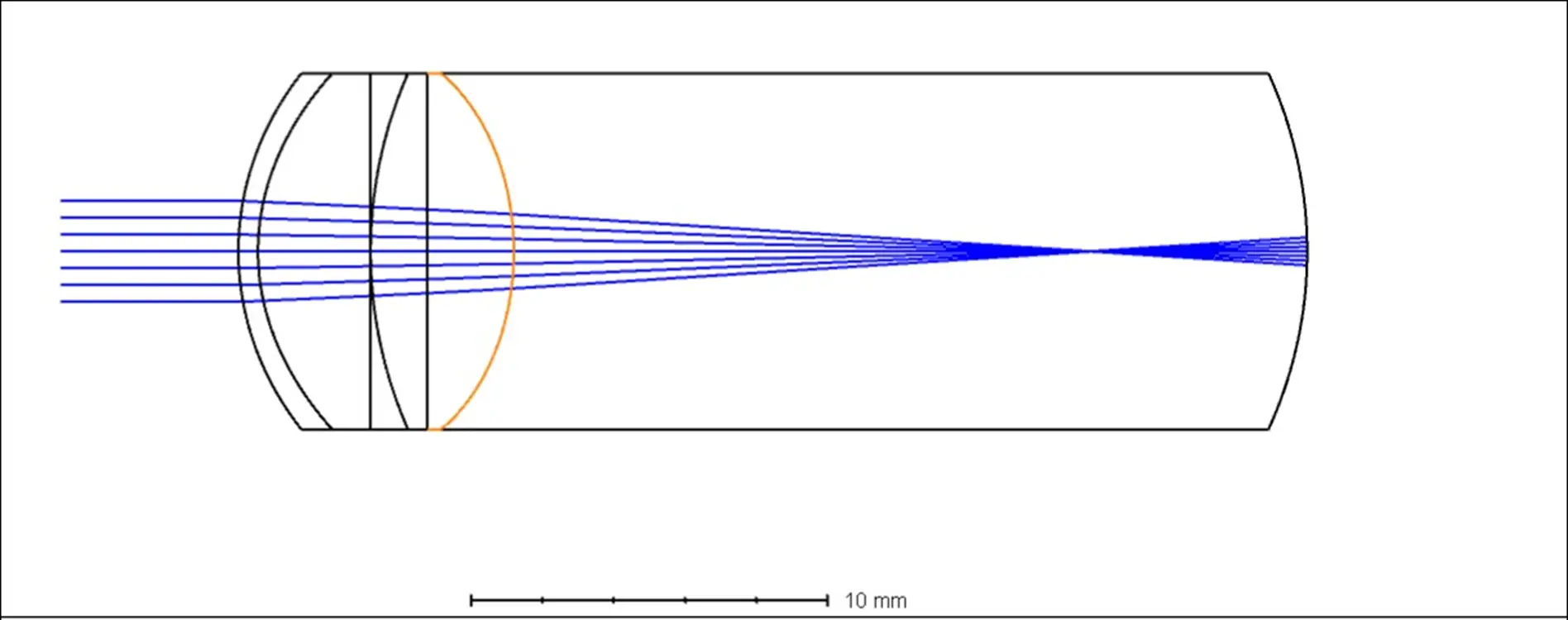
In the case of a myopic (nearsighted) eye, typically the anteroposterior diameter (or axial length) of the eyeball is longer than normal, causing parallel light to focus in front of the retina. As a result, distant objects appear blurred. To bring the light focus onto the retina, the incoming light needs to be made more divergent, which is accomplished by wearing concave lenses. Glasses for myopic individuals are indeed concave lenses.
The human eye is not just a fixed set of lenses. The lens of the human eye can adjust, but this adjustment only increases the refractive power in the optical path, equivalent to adding a convex lens. Therefore, when the myopic eye uses its adjustment power, it still cannot see clearly.
However, when looking at nearby objects, the light emitted from the object is not parallel but divergent. Hence, myopic individuals can see close objects clearly.
Hyperopic Eye
Hyperopic Eye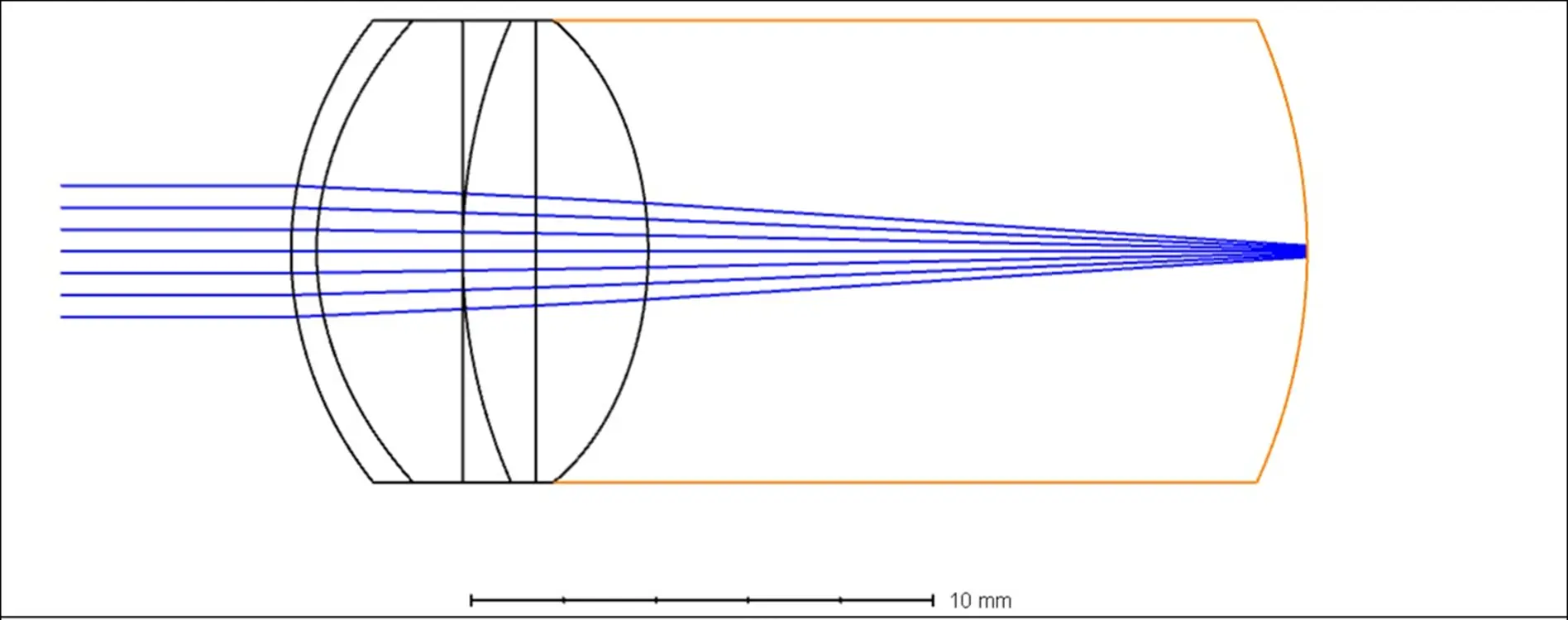
This is the light path of a hyperopic (farsighted) eye. Possibly due to the eyeball being shorter than normal, parallel light focuses behind the retina.
To bring the light focus onto the retina, the incoming light needs to be made more convergent, which is accomplished by a convex lens. Therefore, glasses for hyperopic individuals are typically convex lenses.
When the human eye uses its adjustment power, it can increase the refractive power of the lens. Therefore, hyperopic individuals, under the condition of using adjustment power, may be able to see distant objects clearly. However, if the individual does not actively use their adjustment power, they will have trouble seeing distant objects. Hence, hyperopic individuals struggle to see distant objects clearly.
When looking at nearby objects, the light emitted from the object is divergent, requiring stronger convergence to focus the light onto the retina. This can be achieved by increasing the refractive power of the convex lens or by the individual using more adjustment power. If the individual does not actively use their adjustment power, they will have even more difficulty seeing close objects. Therefore, hyperopic individuals struggle to see nearby objects clearly, unless they strive to see and use their adjustment power.
The Process of Emmetropization in Eyeball Growth
When the eyeball is born, it is smaller than the adult size. It gradually grows larger, and the axial length gradually increases. This is similar to height growth, but far more precise. When does the eyeball stop growing? It is when it grows from a shorter axial length (hyperopic) to just the right axial length (emmetropic). The retina constantly "detects" the focus of objects. If it finds that the focal point is "behind" it, it will ask the axial length to continue to grow. How the retina detects the focal point, how it issues commands, and how the eyeball responds is not yet very clear.
What is known is that if the light input is cut off, the retina does not know when to "stop", so the eyeball will continue to grow. For example, if one half of a monkey's eye is covered (poor monkey
), it has been found that the corresponding half of the eyeball will be larger.
Eye Growth
(Image from The Charles F. Prentice Award Lecture 2010: A Case for Peripheral Optical Treatment Strategies for Myopia)
At the same time, the retinal areas that can command eyeball growth are not equal. The macular fovea, the area of the retina where vision is clearest, has a weaker "voting right" and less influence (determined through experiments where a laser was used to remove retinal area within a 10-degree visual angle in monkey eyes, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2709928/, poor monkeys). However, the retinal area 10-20 degrees from the center has significant authority, especially the retinal area at the 15-degree position, which has the strongest influence (found through experiments where monkeys were made to wear special glasses https://pubmed.ncbi.nlm.nih.gov/32942214/).
Principle of Optical Myopia Control
In an uncorrected myopic eye, or a myopic eye corrected with ordinary frame glasses, the "optimal image plane" formed by light rays entering at different angles is located behind the peripheral retina.

(Left 1, Left 2 in the picture)
As mentioned before, the peripheral retina has the decision-making power on the growth of the eye axis. When it detects that the light rays shining on it always focus behind it, it will issue commands to elongate the eyeball, leading to an increase in myopia.
So, the method to control the rapid increase of myopia is to make sure that the light focused on the peripheral retina must focus in front of the retina, forming so-called peripheral myopic defocus, as demonstrated in the far-right diagram in the picture above. This can control the progression of myopia. By "control", we mean in comparison with wearing regular frame glasses. For instance, if a wearer of regular frame glasses experiences a 100-degree increase in myopia per year, and by wearing glasses that can produce peripheral myopic defocus, the myopia only increases by 40 degrees per year, then there is a 60% control effect.
Optical Control of Hyperopia
It is easy to imagine that if we can make the light focused on the peripheral retina focus behind the retina, forming peripheral hyperopic defocus, can we then make the eye axis grow more quickly, thereby treating hyperopia?
In 2016, such experiments were initiated. You can find an experiment with the code NCT02686879 on clinicaltrials.
The experiment design is disclosed in the 2018 paper Effect of Peripheral Defocus on Axial Eye Growth and Modulation of Refractive Error in Hyperopes: Protocol for a Nonrandomized Clinical Trial:
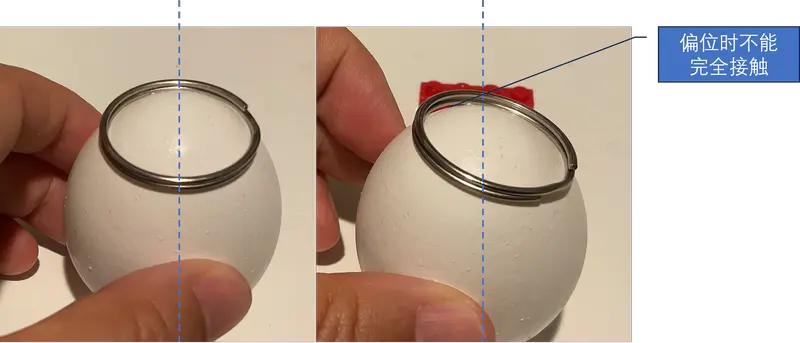
The experimenters used a type of bifocal contact lens.

This contact lens has a more "negative" refraction at the periphery than at the center, thus forming the peripheral hyperopic defocus shown in the picture. Contrary to controlling myopia with peripheral myopic defocus, theoretically, hyperopia should also be controllable with peripheral hyperopic defocus.
According to the record of experiment NCT02686879 on clinicaltrials, the collection of patients was completed in March 2020, and the experiment was completed in February 2022. However, the results of this seemingly straightforward experiment have not been published on clinicaltrials as of June 2023.
Ah, ah, how embarrassing.

photo by Meg Jerrard on Unsplash
Experimental Results
I conducted a literature search using the experiment and the corresponding author of the paper, Nicola S Logan, as keywords. I found:
- Published in February 2022:
The effect of peripheral defocus on axial growth and modulation of refractive error in hyperopes - Published in April 2023:
Effect of peripheral defocus on axial growth and modulation of refractive error in children with anisohyperopia
These two papers.
In the 2022 paper, the experimental method mentioned "The programme of research was registered as a clinical trial: ClinicalTrials.gov NCT02686879", which looks to be the NCT02686879 experiment. Similarly, in the 2023 paper "The programme of research was registered as a clinical trial: ClinicalTrials.gov NCT02686879.", it's also NCT02686879, so it appears to be the same study.
In the 2022 paper, 28 patients were recruited, but a total of 22 participants completed the trial. The intervention group consisted of 11 individuals (8 females and 3 males), with baseline ages ranging from 8.42 to 13.5 years, averaging 11.13 years (SD 1.72); these data were normally distributed (Z = 0.17, P = 0.20). The control group included 11 participants (9 females and 2 males), with ages ranging from 8.33 to 13.92 years, averaging 11.42 years (SD 2.23).
In the 2023 paper, 11 participants, with an average age of 10.56 years (SD 1.43; range 8.25-13.42), completed the trial.
The eye axis measurement device used was also the IOLMaster 500.
Translation into English
In the 2022 paper, the experimental method mentioned "The programme of research was registered as a clinical trial: ClinicalTrials.gov NCT02686879", which seems to be the NCT02686879 experiment. Similarly, in the 2023 paper "The programme of research was registered as a clinical trial: ClinicalTrials.gov NCT02686879.", it's also NCT02686879, so it appears to be the same study.
In the 2022 paper, 28 patients were recruited, but a total of 22 participants completed the trial. The intervention group consisted of 11 individuals (8 females and 3 males), with baseline ages ranging from 8.42 to 13.5 years, averaging 11.13 years (SD 1.72); these data were normally distributed (Z = 0.17, P = 0.20). The control group included 11 participants (9 females and 2 males), with ages ranging from 8.33 to 13.92 years, averaging 11.42 years (SD 2.23).
In the 2023 paper, 11 participants, with an average age of 10.56 years (SD 1.43; range 8.25-13.42), completed the trial.
The device used for measuring the eye axis was the IOLMaster 500 in both cases.
I apologize as I initially misread these two papers when writing this article the first time. After being corrected by a friend, I revisited these two papers. Here is a summary.
While these two papers discuss the same clinical experiment, the content is different, with the most important difference being the subjects of the experiment:
- In the 2022 paper, the intervention group and the control group are two separate groups of people, and both eyes of the individuals in the intervention group wore bifocal contact lenses.
- In the 2023 paper, the intervention group and the control group consist of the same individual's two eyes. The intervention group is the eye with the higher degree of hyperopia in the subject, and this single eye wore a bifocal contact lens.
The other parts of the experimental design are almost the same:
- The eye axis measurement was done using the IOL Master 500.
- The intervention time ranged from 6 to 30 months, a period of two years, followed by a 6-month cessation of intervention.
Let's compare the result graphs describing the same NCT02686879 clinical experiment:
First, the changes in the eye axis:
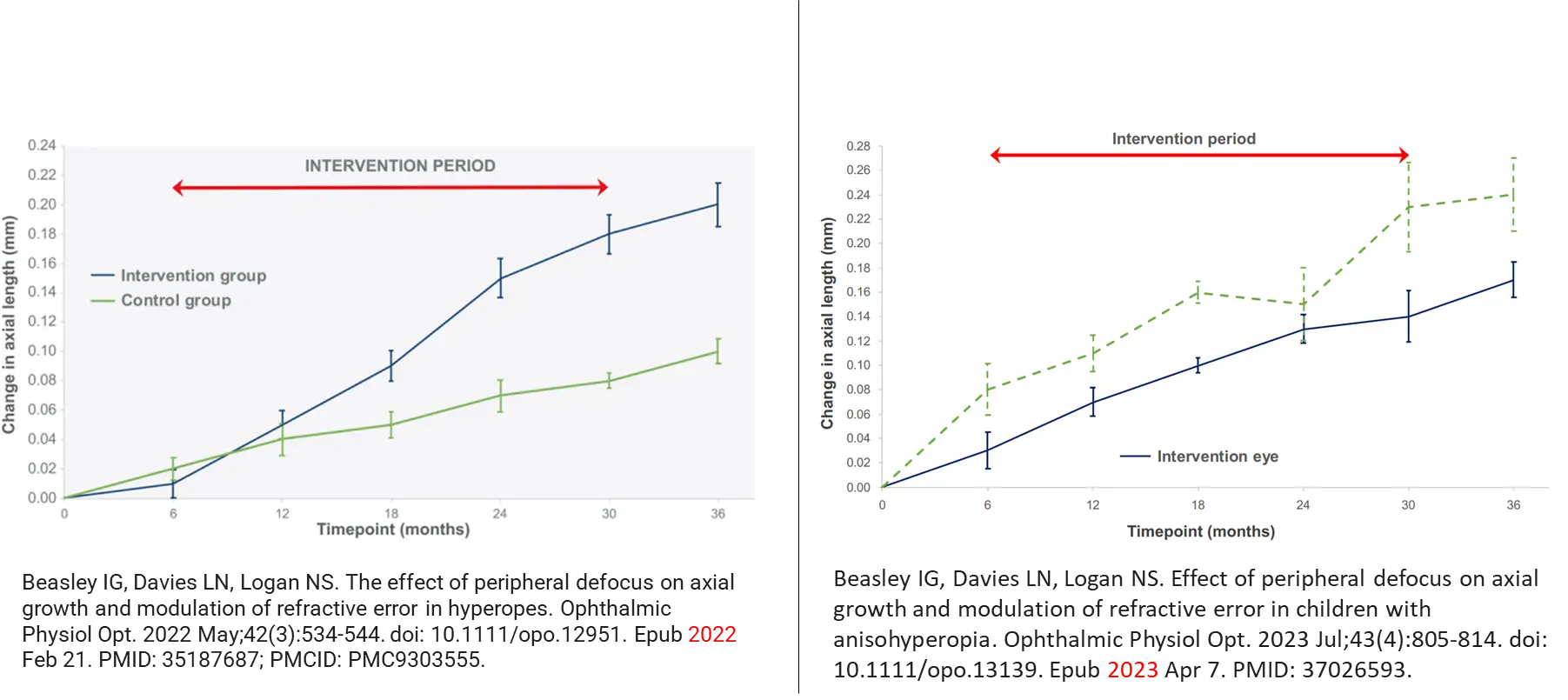
For the eye axis, both in the 2022 and 2023 papers, there was a statistically significant difference in the changes in the eye axis, with wearing bifocal contact lenses.
Next, the changes in refraction:
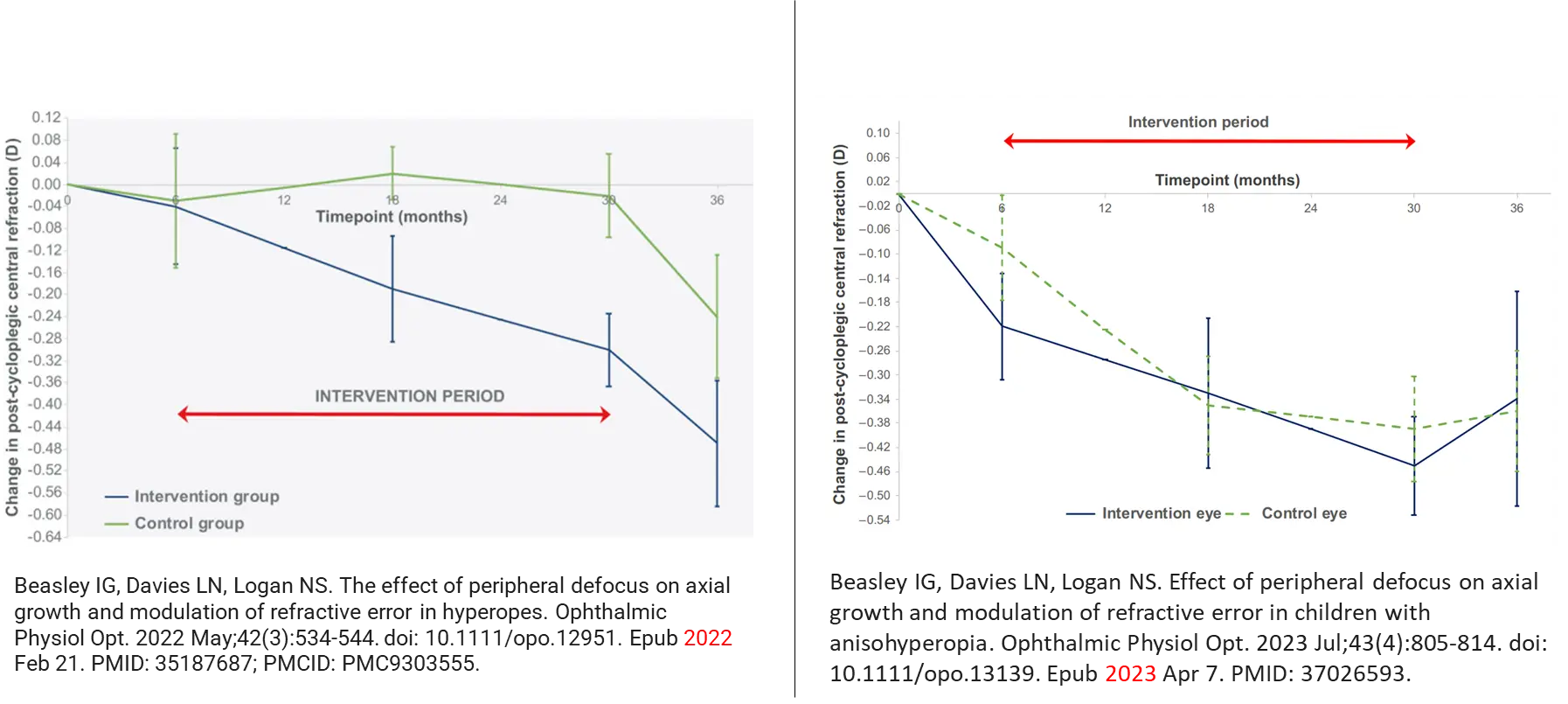
However, for the change in refraction, in the 2022 experiment, although the graph shows a large difference between the two groups, after statistical analysis, it did not reach a level of significant statistical difference.
However, although the mean values showed a greater reduction in post‐cycloplegic refractive error in those receiving the intervention compared to the control group, this did not reach a level of significance nor achieve adequate statistical power.
In the 2023 experiment, which was a within-subject control experiment, the curves of refractive changes were almost completely overlapped.
This suggests that the use of bifocal contact lenses to form peripheral hyperopic defocus can cause some growth in the eye axis, but this is likely of little clinical significance.
Discussion
I propose:
Only those who are incapable of becoming myopic, will not become myopic!
A corollary: Hyperopia cannot simply be controlled by increasing myopia!
Take a moment to look at yourself in the mirror or glance at the people around you; myopia is ubiquitous. Controlling myopia has only become possible in recent years, but there are countless ways to increase myopia. These include, but are not limited to, reading novels under the dim light of a flashlight while hidden under the bed covers (this method might be a bit dated), or playing games on a phone or tablet while under the covers, writing so closely to the table that your nose can smell the ink...
This type of close-range, prolonged eye usage can produce a very strong peripheral hyperopic defocus, far more potent than any bifocal contact lenses. If a person can maintain non-myopia under such environmental influences, they are already exceptional. If he/she is still hyperopic, do you believe he/she could control hyperopia by employing "reverse" methods of myopia control?
There's a famous quote in the book "Internal Medicine" that can explain the cause of any disease: Environmental factors act on genetically susceptible individuals. For myopia, no less than 80% of high school graduates in large cities are myopic. The number of individuals with myopia far exceeds those without it. Studying the causes of myopia at this stage isn't very meaningful; it would be more valuable to examine those non-myopic individuals. What enables these individuals to maintain non-myopia amidst widespread myopia caused by environmental factors? I believe this is a case of environmental factors acting on genetically non-susceptible individuals. Non-myopic individuals must have strong genetic traits. Among these non-myopic individuals, the hyperopic are an even more non-myopic group. Therefore, in the pathogenesis and disease development of hyperopia, the influence of genetics might be stronger, robust enough to resist the influence of environmental factors. Simply using peripheral hyperopic defocus as an environmental factor acting on hyperopia is probably insufficient. We likely need to continue to seek new therapeutic targets.
References
- The Charles F. Prentice Award Lecture 2010: A Case for Peripheral Optical Treatment Strategies for Myopia
- Eccentricity-dependent effects of simultaneous competing defocus on emmetropization in infant rhesus monkeys
- NCT02686879
- Effect of Peripheral Defocus on Axial Eye Growth and Modulation of Refractive Error in Hyperopes: Protocol for a Nonrandomized Clinical Trial
- The effect of peripheral defocus on axial growth and modulation of refractive error in hyperopes
- Effect of peripheral defocus on axial growth and modulation of refractive error in children with anisohyperopia